



Scrotal ultrasound remains an indispensable diagnostic method for evaluating the scrotum due to its ability to show anatomical detail well. It is relatively fast, relatively inexpensive, can quickly lead to a diagnosis based on the patient’s symptoms, and most importantly, does not involve ionizing radiation.
Normal Scrotal Anatomy and Examination Technique
Both testicles are suspended within the scrotum by the spermatic cord. The visceral layer of the tunica vaginalis covers the testis, while the parietal layer forms the scrotal wall. Normally, there is about 2-3 mL of fluid between the two layers.
The testis measures approximately 3-5 cm in length, 3 cm in anterior-posterior diameter, and 2-4 cm in width, with a weight of about 12-19 grams. The head of the epididymis is located at the upper lateral part of the testis, is triangular in shape, and measures less than 1 cm in diameter. The epididymis is 6-7 cm in length, with the head being the widest part.
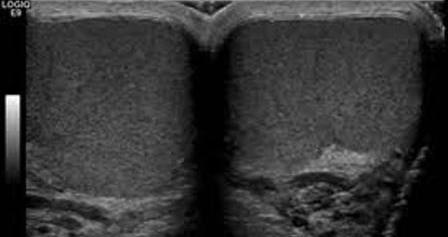
The scrotum should be examined sonographically using high-frequency linear probes and proper user settings. Sonographically, a normal testis has a slightly echogenic and homogeneous internal structure (Image 1). In the presence of intrascrotal fluid, the tunica albuginea appears slightly echogenic, and the mediastinum testis appears more echogenic. The epididymis has a homogeneous appearance with an echogenicity similar to that of the testis.
Image 1. Sonographic appearance of a homogeneous slightly echogenic testicular parenchyma in axial plane and the echogenic mediastinum testis (arrow).
Scrotal Trauma
Due to its anatomical location, scrotal trauma accounts for less than 1% of injury-related traumas. It most commonly occurs between the ages of 10 and 30. Traumas can be blunt, penetrating, thermal, or involve skin injuries.
Trauma can lead to scrotal or testicular edema, hematoma, hematocele, hydrocele, torsion, fracture, or rupture. In trauma cases, ultrasound is an ideal method as it can non-invasively show the contents of the testis, blood flow, scrotal hematoma, other fluid accumulations, and foreign bodies.
Infertility
In the evaluation of infertility, ultrasound is used to assess testicular size, positioning, and the presence of subclinical varicocele, which is often accompanied by atrophy.
In cryptorchidism (undescended testis), ultrasound is useful, especially in demonstrating the testis within its most common location, the inguinal canal, or if it is located at the external orifice of the canal. In these locations, ultrasound is the imaging method of first choice. Sonographically, an undescended testis is smaller and has decreased echogenicity compared to a normal testis. The longer the duration, the more pronounced the atrophy and hypoechoic appearance.
Microlithiasis
Testicular microlithiasis is observed in 5% of the population between the ages of 17 and 35. It is often associated with infertility, cryptorchidism, and testicular cancer. These are intratubular calcifications measuring 1-2 mm in size. The presence of 5 or more calcifications in each ultrasound field is considered pathological.
Scrotal Masses
Extratesticular Masses
Simple cysts of the epididymis and spermatocele are the most common extratesticular masses and are generally asymptomatic. Epididymal cysts are most often located at the head of the epididymis, but can also be seen in the body and tail. Spermatocele is usually larger than epididymal cysts.
Intratesticular Masses
Cystic Lesions
Non-neoplastic cystic lesions are frequently detected in routine testicular examinations, and most of them are benign. These lesions are easily recognized in ultrasound due to their appearance, location, and cystic nature. Tunica albuginea cysts, simple testicular cysts, rete testis ectasia, intratesticular varicocele, intratesticular abscess, and epidermoid cysts fall under this group.
Solid Lesions
When a scrotal mass is detected on physical examination, the priority is to determine whether it is intratesticular or extratesticular. The majority of extratesticular masses are benign, whereas most intratesticular solid masses are considered malignant until proven otherwise.
Therefore, the primary purpose of imaging is to determine the location (inside or outside the testis) and the nature (cystic or solid) of the mass. Testicular masses of malignant nature are generally hypoechoic compared to adjacent parenchyma. Hemorrhage and calcifications within the mass can create a hyperechoic appearance.
Tumor-like Lesions
A mass detected within the testis does not always indicate the presence of a tumor. Orchitis, hemorrhage, ischemia, or infarction are non-neoplastic pathologies that can mimic testicular tumors. These lesions have poorly defined borders compared to testicular masses but may present with overlapping findings.
Scrotal Ultrasound Prices 2026
For information on scrotal ultrasound prices for 2026, you can contact us immediately.
What is the cost?
Dr. Abdullah Cevahir
Radiology Specialist
Hekimoğlu Imaging and Diagnostic Center