



Retrograde urethrography is considered the best initial study for imaging the male urethra and periurethral region, and it is indicated for the evaluation of urethral injuries, strictures, and fistulas.
Male urethral abnormalities are a common problem that manifest with significant clinical symptoms and can lead to quality-of-life issues for those affected. Although these abnormalities can occur at any age, there is a marked increase in men over the age of 55.
The causes of urethral abnormalities are generally categorized as iatrogenic, infectious, and/or inflammatory, traumatic, or neoplastic. The long-term sequelae from these abnormalities often result in obstruction due to urethral stricture disease; however, additional complications include incontinence and impotence.
An iatrogenic cause, such as instrumentation from transurethral resection of the prostate, is one of the leading causes of stricture disease and accounts for 45% of strictures. Urethral trauma frequently occurs in patients with pelvic trauma and can lead to significant long-term morbidity if untreated.
Regardless of the cause of urethral abnormalities, imaging studies are generally used complementarily and play an important role in the comprehensive evaluation of the urethra because imaging can reveal pathological findings that are not visible in urethroscopy.
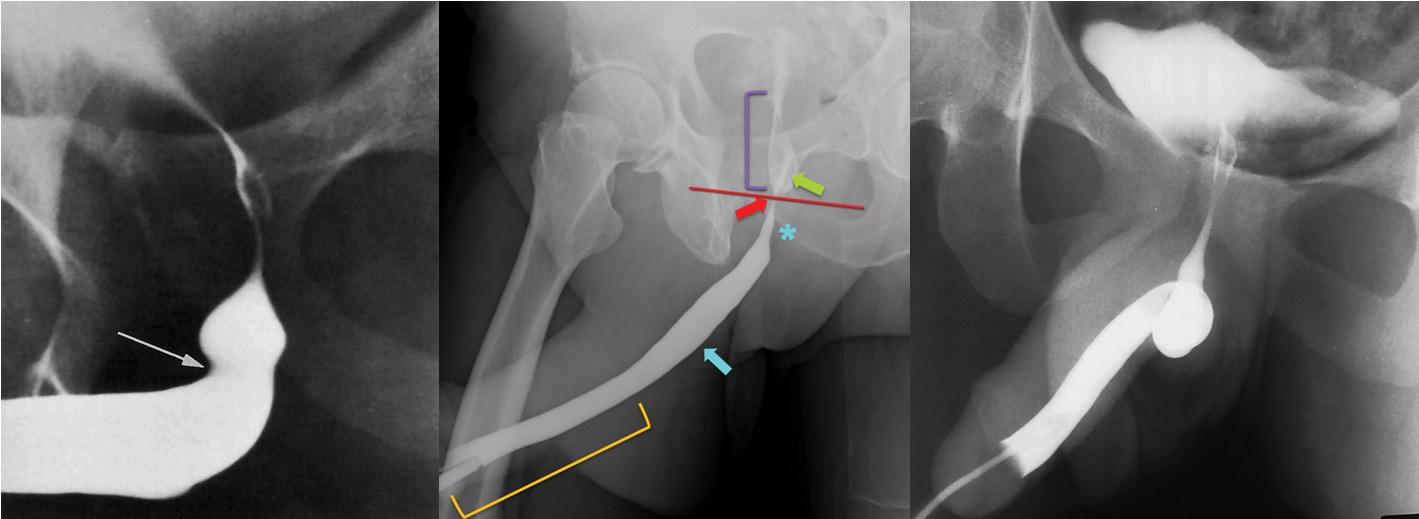
Retrograde urethrography and voiding cystourethrography (VCUG) are considered standard imaging techniques for evaluating urethral abnormalities. While retrograde urethrography (Figure 1) is the reference standard for evaluating the anterior urethra, the posterior urethra and bladder are better evaluated in VCUG images.
Figure 1. The retrograde urethrogram image shows normal urethral anatomy. Penile urethra (orange bracket), bulbar urethra (blue arrow), normal narrowing of the bulbar urethra at the bulbomembranous junction (*), membranous urethra (red arrow), urogenital diaphragm (red line), prostatic urethra (purple bracket), and verumontanum (green arrow).
How Is A Retrograde Urethrography Test Performed?
It is performed by direct opacification of the urethra with contrast material. The external meatus is prepared in a sterile manner. When the balloon part of the catheter is seated in the fossa navicularis of the penile urethra, the balloon is inflated with 1.0-1.5 mL of saline solution. Lubricant is not recommended, as it may prevent the balloon from staying in place.
The patient is placed in a supine 45° oblique position. The penis should be placed laterally on the proximal thigh. The patient should be informed about the mild discomfort that will be experienced during balloon inflation. Then, under fluoroscopic guidance, 20-30 mL of 60% iodinated contrast material is injected to fill the anterior urethra.
Spasm of the external urethral sphincter is commonly encountered, which prevents the deep bulbar, membranous, and prostatic urethras from filling. To overcome this resistance, slow, gentle pressure is usually required. After the contrast material is seen passing into the bladder, spot radiographs are obtained.
If the contrast material is properly applied, the contrast can be seen spurting from the bladder neck into the bladder.
Looking at Urethral Anatomy;
The urethra is examined in two sections: proximal and distal. The proximal urethra consists of prostatic and membranous segments. The prostatic urethra is divided into two segments: the proximal prostatic urethra and the distal prostatic urethra, separated by the verumontanum, with an angle of approximately 35 degrees.
The verumontanum appears as an oval filling defect in the posterior aspect of the prostatic urethra. The distal end of the verumontanum marks the proximal boundary of the membranous urethra, which is approximately 1 cm long and passes through the urogenital diaphragm. This is also the region of the external urethral sphincter.
The narrowest segment of the urethra is the membranous urethra, which can reach a diameter of 6-7 mm during voiding. Internal and external sphincters are also seen at the level of the proximal urethra. The distal boundary of the membranous urethra is where the bulbar urethra takes on a conical shape.
Identification of the bulbomembranous junction in retrograde urethrography is crucial for evaluating patients with urethral disease and for planning urologic procedures. When the posterior urethra is optimally opacified and the verumontanum is visible, the bulbomembranous junction is located 1–1.5 cm distal to the lower edge of the verumontanum.
When the posterior urethra is opacified, the bulbomembranous junction can be localized where an imaginary line connecting the lower edges of the obturator foramina intersects the urethra.
Strictures in Retrograde Urethrography
The anterior urethra extends from the end of the membranous urethra to the urethral meatus. It is divided into two segments: the bulbar (most proximal) segment and the penile (pendulous) segment. There is usually a slight angulation of the urethra at the point where these two segments join at the penoscrotal junction.
Contraction or spasm of the constrictor nude muscle, which is a deep musculoskeletal sling of the bulbocavernosus muscle, can cause proximal anterior indentation of the urethra in retrograde urethrography, or less frequently, circumferential indentation. This circumferential urethral indentation should not be mistaken for a urethral stricture (Figure 2).
If the membranous urethra can be identified, it will not be confused with a stricture. Narrowing elsewhere in the urethra will be clearly identified separately from the membranous urethra and thus represents a pathological stricture. If the patient is not adequately positioned obliquely, the bulbar urethra will appear short and will not be adequately evaluated (Figure 3).
Filling of the Cowper’s ducts should not be misinterpreted as extravasation (Figure 3). Opacification of the prostatic ducts, Cowper’s ducts, and periurethral Littré glands is typically, but not necessarily, associated with urethral inflammatory diseases and strictures.
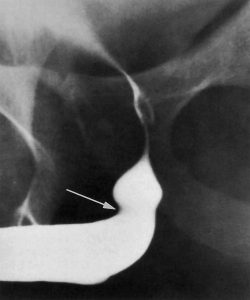
Figure 2. Retrograde urethrogram shows a focal smooth indentation (arrow) at the anterior side of the proximal bulbar urethra by the compressor nude muscle.
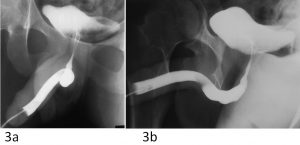
Figure 3. The effect of patient positioning on urethral appearance during retrograde urethrography. (a) Retrograde urethrogram obtained with the patient lying supine shows the bulbar urethra as a cystic structure resembling a diverticulum. (b) Retrograde urethrogram obtained after the patient was placed in an upright oblique position with the penis stretched shows a normal appearance of the penoscrotal junction and bulbar urethra.