



Celiac Trunk Color Doppler Ultrasound
The celiac artery, also called the celiac trunk, is the first major visceral branch of the abdominal aorta. It originates from the anterior aortic surface between the diaphragmatic crura. Shortly after its origin, approximately 1 to 3 cm away, it bifurcates into the common hepatic and splenic arteries, which are easily visualized via ultrasound. The celiac artery also gives rise to the left gastric artery, although this branch is generally not seen sonographically. The branching pattern of the celiac artery is quite consistent and observed in approximately 93% of individuals. In the most common variations, one or more branches of the celiac artery arise separately from the aorta or the superior mesenteric artery (SMA). In less than 1% of individuals, the celiac artery and SMA share a common trunk that originates from the aorta, bifurcating into the celiac artery and SMA within 1 or 2 cm of the aorta.
How Is Celiac Trunk Color Doppler Ultrasound Performed?
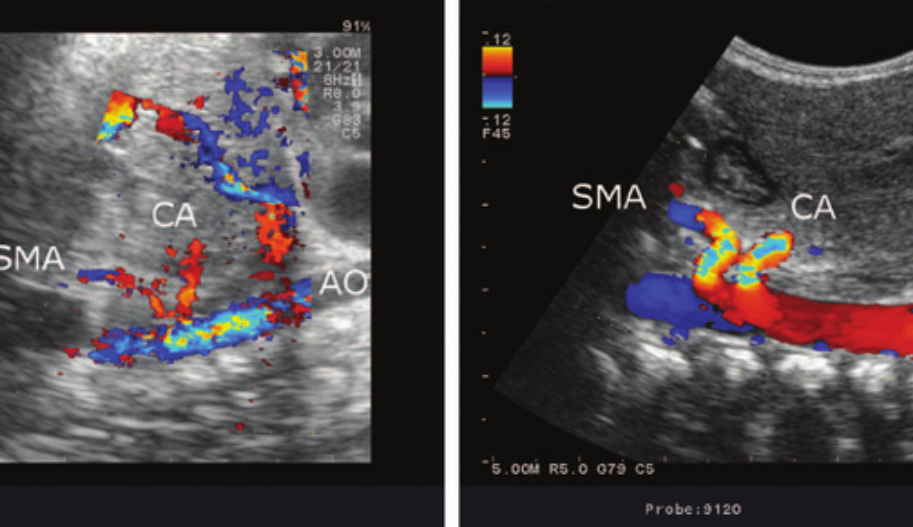
The color Doppler ultrasound examination of the celiac artery typically begins with a transverse scan of the proximal abdominal aorta. The transverse approach often shows the bifurcation of the hepatic and splenic branches, resembling a “T” or a “seagull” appearance. For evaluating the origin of the celiac artery, a longitudinal approach is preferred. This view also allows for the evaluation of the SMA, which lies just below the celiac artery.
Normal Values for Celiac Trunk Color Doppler Ultrasound
The characteristic Doppler waveform of the celiac artery shows a low-resistance flow pattern. As mentioned earlier, continuous forward flow throughout diastole is necessary for adequate perfusion of the liver and spleen. The Doppler waveforms of the hepatic and splenic arteries also display this low-resistance pattern. The normal range of blood flow velocity in the celiac artery is between 98 and 105 cm/s.
The mesenteric circulation is notable for its wide arterial anastomoses and rich collateral network. This network allows for continuous circulation to splanchnic organs in the event of stenosis or occlusion of the mesenteric branches, avoiding end-organ ischemia. With celiac artery occlusion, collateralization occurs through the pancreaticoduodenal artery arcade, a network of small vessels surrounding the pancreas and duodenum. These vessels enlarge and feed the gastroduodenal artery. In cases of proximal celiac artery occlusion, retrograde flow from the gastroduodenal artery supplies the main hepatic artery, thus ensuring blood supply to the liver and spleen.
Splenic Artery
The splenic artery follows a tortuous path along the posterosuperior border of the pancreas body and tail, terminating in a series of branches at the splenic hilum. Along its course, the splenic artery gives off several pancreatic branches, gastric branches, and the left gastroepiploic artery. These vessels are typically not seen on Doppler ultrasound.
Hepatic Artery
The hepatic artery is the branch of the celiac artery that runs to the right of the patient. After traveling a short distance along the superior border of the pancreas head, the main hepatic artery gives rise to the gastroduodenal artery branch, which is often visible on ultrasound at the anterosuperior border of the pancreas head.
The hepatic arteries are typically well visualized sonographically via an anterior abdominal approach. The common hepatic artery is easily identified where it originates from the celiac artery. The right and left hepatic artery branches can be traced from the porta hepatis into the liver. As previously mentioned, the hepatic artery system exhibits low-resistance flow characteristics, with continuous forward flow during diastole. It is important to note that blood flow in both the proper hepatic artery and the portal vein is hepatopetal, meaning that it flows toward the liver. This may be the only location where the accompanying artery and vein display blood flow in the same direction.